Pathogenesis of Retinopathy of Prematurity
Does Inflammation Play a Role?
NAINR. 2013;13(4):161-165.
Abstract and Introduction
Abstract
Retinopathy of prematurity (ROP) is a disorder of retinal–blood vessel development that is potentially blinding. ROP is the number one cause of blindness in infancy and the second leading cause of childhood blindness in the Unites States. The exact etiology is not completely understood and many factors appear to contribute to the pathogenesis and progression of the disease. These factors may include prematurity, low birth weight, genetic predisposition, oxygen, hypoxia, ischemia, insulin-like growth factor, vascular endothelial growth factor and sepsis. This article reviews the process of retinal development, the pathogenesis of ROP and how oxidative stress, infection and inflammation may contribute this pathogenesis.
Introduction
Retinopathy of prematurity (ROP) is a disorder of retinal–blood vessel development and is the second leading cause of childhood blindness in the United States behind cortical visual impairment.[1] The National Center for Health Statistics report has listed the incidence of infants born at risk for developing this eye disease (≤ 32 weeks' gestation) to be at 2% of all live births. In 2008, 84,224 babies were born at or less than 32 weeks' gestation in the United States.[2] The National Eye Institute has estimated that 14,000–16,000 of these infants are affected by some degree of ROP and that 1100–1500 infants in the United States develop ROP that is severe enough to require medical treatment on an annual basis. Of these, 400–600 become legally blind from ROP each year.[3]
Retinopathy of prematurity (ROP) is a potentially blinding disorder caused as abnormal new blood vessels develop in the immature retina. In 1942, an ophthalmologist from Boston named Theodore Terry was the first to recognize a previously undescribed form of blindness in children born prematurely and of low birth weight. He named the condition based on the eye examination finding that showed a white fibrous mass behind the lens which obliterated the retinal vessels—"retrolental fibroplasia."[4] The name was later changed in 1984 by consensus of an international group of pediatric ophthalmologists to retinopathy of prematurity.[5]
Despite efforts to avoid the development of ROP since it was first recognized in the 1940s by Terry, ROP continues to be a challenging problem in the care of premature infants. The exact etiology of ROP is not completely understood and many factors appear to contribute to the pathogenesis and progression of the disease. Prematurity, genetic predisposition, oxygen, hypoxia, ischemia, insulin-like growth factor 1 (IGF-1) and VEGF all have been shown to be important in the development of ROP.[6]Severity of illness, sepsis, acidosis, blood transfusions and light have also been associated with ROP.[7] The degree of prematurity itself remains the most significant risk factor, with the avascular retina of premature babies being at the highest risk.[8,9] High oxygen saturations, oxygen fluctuation and hypoxia are known to significantly contribute to the development of ROP.[8,10-16]
Normal Retinal Development
The vascular supply for the retina consists of two main parts: (1) the choroidal vessels that underlie the retina and (2) the retinal vessels that serve the inner retina. Vascular development for the choroid is complete by 22 weeks of gestation.[17] The choroid provides nutrition through diffusion to the early retina. The choroidal vessels are more permeable and have a high venous partial pressure of oxygen (PaO2). They lack the ability to autoregulate in response to hyperoxia. Therefore, during times of hyperoxia, PaO2 levels are raised across the thickness of the retina and the retinal vessels respond by constricting.[7] As the retina matures, there is little change in the choroid blood supply despite the high rate of growth and development in the retinal during mid to late gestation. As a result, the retina requires its own vascular supply for adequate nutrition.[18] Normal retinal vascular development begins at the optic disk at about 16 weeks' gestation through a process of vasculogenesis. Vasculogenesis is the de novo development of vasculature that involves the proliferation, differentiation, and organization of blood vessels from endothelial progenitors—angioblasts.[17] To accomplish vasculogenesis, circulating angioblasts develop early retinal vessels in the region surrounding the optic nerve. Angiogenesis then proceeds to extend the retinal vasculature to the periphery by 36–40 weeks' gestation through formation of new blood vessels from existing vessels.[19,20]
The developing retinal vessels reach only 70% of the distance from the optic disk to the periphery by 27 weeks of gestation.[7] Retinal vascular development is ideally accomplished while the fetus is in the uterus in a relatively hypoxic environment where the average PaO2 is 25–35, which is supported by the infant's fetal hemoglobin and lower metabolic demands.[18]
The retinal vasculature comprises two laminar but interconnected layers: the primary superficial layer and the ganglion cell layer which lies deeper in the retina. The layers are joined by fine capillaries.[21] Vasculogenesis in the retina is believed to be responsible for early vessel formation in the inner plexus but is not responsible for vessel formation in the temporal and peripheral regions of the human retina.[21] The formation of the primary vascular layer in the retina is intimately associated with the development of cells in the nerve fiber/ganglion region known as astrocytes.[22,23] Astrocytes are glial cells that give biochemical support to endothelial cells, sense physiologic hypoxia and express vascular endothelial growth factor (VEGF).[24] VEGF is one of the most important factors in vascular development and is associated with pathologic angiogenesis.[9,20,24] Astrocytes emerge from the optic nerve and migrate just ahead of the developing vascular network.[25] This places them in a position to respond to physiologic levels of hypoxia in the avascular areas of retina.[18,23,26] Astrocytes are present only in retinas in which retinal vasculature forms, and are restricted to the inner layer of retina that allows them to respond to hypoxia of the inner layers by expressing VEGF which is essential to induce the formation of the superficial layer of blood vessels.[23,27] The normal formation of retinal vessels depends on a period of physiologic hypoxia to stimulate the release of VEGF by the astrocytes.[18,26,28,29] Hyperoxia, will inhibit new blood vessel formation by down-regulating VEGF expression by the astrocyte, limiting the hypoxic stimulus.[23,30] This down-regulation may cause a delay in the natural retinal development. When a fetus is delivered prematurely, the normal processes for the developing retinal vascular bed that will nourish the eye are interrupted.
Insulin-like growth factor (IGF-1) is another key factor in retinal development. IGF-1 is hypothesized to regulate retinal neovascularization through control of VEGF activation. Studies have demonstrated a permissive role for IGF-1 in new blood vessel formation as it allows maximum VEGF stimulation of new vessel growth. Low levels of IGF-1 will inhibit vessel growth despite the presence of VEGF.[6,31,32] IGF-1 is supplied to the fetus from the placenta and the amniotic fluid. Premature birth causes IGF-1 levels to fall through loss of the amniotic fluid and placental supply in the fetal environment.[9]
Pathogenesis
When an infant is delivered prematurely, the retinal development must continue in an altered environment, creating the risk for developing ROP. The infant's retina becomes hyperoxic (even in room air) leading to decreased levels of VEGF and for a time, vasculogenesis is halted between the vascular and avascular retina, increasing the risk for developing ROP.[33,34] Additionally, IGF-1 levels fall from in utero levels after birth, due to the loss of IGF-1 which is provided by the placenta and the amniotic fluid.[9] The disease process for the development of ROP is biphasic with an initial phase of vessel growth retardation followed by a second phase of vessel proliferation.[9]
Phase I
The first phase of ROP has been described as the hyperoxia-vasocessation phase.[35] It occurs from birth to postmenstrual age of 30–32 weeks.[11] When a very low birth weight premature infant is born, the infant's immature lung places them at high risk for hypoxemia. The medical response is to provide increased amounts of fraction of inspired oxygen (FIO2). Under conditions of low retinal metabolic demand this creates relative retinal hyperoxia. Production of VEGF may be inhibited by the high levels of supplemental oxygen the infant may receive in the NICU, which causes cessation of normal retinal growth, and vessel constriction with a potential for vaso-obliteration of new immature vessels. This may cause subsequent death of vascular endothelia cells.[12,30,33,35-38]
In utero, the fetus receives insulin-like growth factor (IGF-1) via the placenta, which ceases at the time of birth. The infant is predisposed to phase 1 ROP due to an inherent lack of normally developed vessels.[19]
After premature birth, IGF-1 is suppressed by poor nutrition, sepsis, and acidosis. Preterm infants with prolonged low serum levels of IGF-1 and slow weight gain, have an increased risk of ROP.[6] A low level of IGF-1 decreases retinal vascular growth by suppressing the VEGF activation necessary for endothelial cell survival.[31] As the infant matures, the non-vascularized retina has increasing metabolic activity leading to tissue hypoxia. This hypoxia promotes increasing levels of VEGF along with increasing IGF-1 to a critical level, which then triggers retinal neovascularization that moves to phase II ROP.[31]
Phase II
The second phase of ROP is the relative hypoxia-revascularization phase. It is characterized by a progressive increase in metabolic activity in the non-vascularized retina resulting in a hypoxia-induced retinal neovascularization. This phase begins around 32–34 weeks' postmenstrual age.[39] Prior to 32 weeks' gestation, the retina is very immature with photoreceptors that are not yet fully functional and the retinal metabolic demand is low.[40] As the retina matures, there is an increased metabolic demand and oxygen consumption, creating a relative retinal hypoxia.[35,41] Hypoxia stimulates the up-regulation of pro-angiogenic growth factors such as vascular endothelial growth factor (VEGF) and erythropoietin, which, in severe cases, leads to uncontrolled vascular growth in the vitreous.[9,11] The changes in retinal tissue oxygenation can be exacerbated by weaning the infant from oxygen therapy and potentially by targeting low oxygen saturation levels. Phase II ROP does not proceed with a gradual transition from avascularized to vascularized retina but rather a demarcated ridge line develops along the retina that separates the central vascularized region of the retinal from the peripheral avascular region. This structure histologically consists of mesenchymal and endothelial cells.[42] Vascular development from this stage may resume without significant disruption, or may progress to significant ROP as seen by an abnormal proliferation of retinal vessels into the vitreous and over the surface of the retina.[43] The new vessel growth is abnormal, producing capillary networks that are fragile, leaky and poorly perfused. These new vessels fail to alleviate tissue hypoxia leading to persistent growth of these abnormal vessels.[44]
Early exposure of the retina to hypoxia and ischemia exacerbate delayed retinal development in premature infants, in part due to low levels of local and systemic growth factors including IGF-1. VEGF production within the retina occurs in response to relative hypoxia but is unable to trigger angiogenesis in the absence of adequate IGF-1. Over time, postnatal levels of IGF-1 recover and reach a critical threshold, and VEGF-induced angiogenesis is triggered, contributing to the occurrence of ROP.[9,44,45,46]
Classification of ROP
ROP is classified first by the location of the lesion of abnormal vascular development relative to the optic nerve (zone), second by the degree of abnormality (stage), third by the presence or absence of dilated and tortuous posterior pole vessels (plus disease), fourth by the extent of the disease (clock hours) and finally by retinal sequelae as the disease involutes. Severity of disease is based on the zone, stage and presence of plus disease.
Zones
There are three zones that describe the extent of retinal vascular development. Zone 1 is the area immediately surrounding the optic nerve and macula, extending from the disk to twice the distance between the disk and the macula, and has the highest risk for the development of scar formation, significant visual impairment, and retinal detachment. Zone 2 is a ring concentric to zone 1 which extends to the nasal ora serrata (the edge of the retina on the side of the eye toward the nose) and may develop lesions that can progress to the above-mentioned significant sequelae. Zone 3 is the remaining crescent of retina on the temporal (toward the temple) side and carries the lowest risk of a poor outcome from severe ROP.[47] See Fig 1.
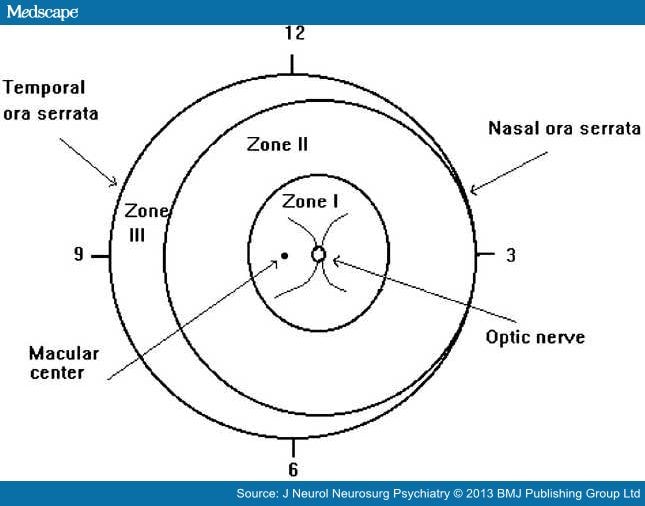
Figure 1.
Scheme of retina of the right eye showing zone borders and clock hours used to describe the location and extent of retinopathy of prematurity.48
Stages
Five stages of abnormal vessel development have been identified in ROP to describe the severity, ranging from mild (stage 1) to severe (stage 5). describes the characteristics of the different stages.
Table 1. Stages of ROP.47,49
| Stage 1 | A line of demarcation between the normal retina nearer the optic nerve and the non-vascularized retina peripherally. |
| Stage 2 | A ridge of scar tissue that arises in the region of the demarcation line that has both height and width. |
| Stage 3 | Severely abnormal blood vessel growth when the vessels grow through the ridge toward the center of the eye (intravitreous) instead of following their normal growth pattern along the surface of the retina. This is the most common stage to begin treatment. |
| Stage 4 | Severely abnormal vessel development with a partial retinal detachment. Stage 4 is divided into two parts: |
| ∠Stage 4A where the detachment does not include the macula, and the vision may be good. | |
| ∠Stage 4B with macula detachment and a marked decrease in vision potential. | |
| Stage 5 | Complete retinal detachment, usually with the retina pulled into a funnel-shaped configuration by the fibrovascular scar tissue. |
Plus Disease
Plus disease implies increased venous dilatation and arteriolar tortuosity of the posterior retinal vessels near the optic nerve. It also includes the growth and dilatation of abnormal blood vessels on the surface of the iris, rigidity of the pupil, and vitreous haze. The diagnosis of plus disease is usually made on the appearance of the vessels near the optic nerve, as compared with standard retinal photographs. The presence of plus disease suggests a more fulminant or rapidly progressive course. Rush disease is the term used to define ROP in zone 1 that also has plus disease. Patients with rush disease tend to have a poorer prognosis than other eyes with ROP.[47]
Oxidative Stress and ROP
ROP was first associated with oxygen supplementation in premature infants in the 1940s. Higher oxygenation is associated with the development of abnormal vascular growth in the eye.[50] Because ROP has been related to hyperoxia, there is concern that reactive oxygen species (ROS) may be involved in this disease but there is limited information to prove or disprove the role of oxidative stress in ROP.[41] Very high concentrations of the free oxygen radical generator, hypoxanthine, have been found by autopsy in the eyes of babies at risk of developing ROP.[51] It has also been found that those retinas are low in several antioxidants and antioxygenzymes in the rat model.[52] Premature human retinas have been found to have relatively low levels of retinal vitamin E but contain an abundance of retinal vitamin C.[53] The premature infant has inadequate concentrations of antioxidants at birth, as well as an impaired ability to synthesize antioxidants in response to hyperoxia making them susceptible to ROS-induced damage that may lead to ROP.[54]
Oxygen has been identified as a key element in the delay in retinal maturation and in the development of ROP. Vascular endothelial growth factor (VEGF) is an oxygen-mediated factor that is essential for normal retinal vessel growth. As the retina develops anterior to retinal vessels, there is an increase in oxygen demand from the developing neural tissue that creates localized hypoxia. VEGF is expressed in response to this hypoxia and blood vessels grow toward the VEGF stimulus. When an infant is born prematurely, the oxygen environment is altered from levels in the uterus. The retina becomes relatively hyperoxic which will cause vasoconstriction, vaso-obliteration and will inhibit new blood vessel formation by down-regulating VEGF expression.[55] This may cause a delay in the natural retinal development or increase the risk of developing ROP. Insulin-like growth factor-1 (IGF-1) has also been associated with ROP as a necessary factor for the function of VEGF. The infants' supply of IGF-1 from the placenta and amniotic fluid is removed at the time of birth contributing to the retinal vasculature going dormant. As the infant matures, IGF-1 levels may be slow to elevate and must reach a threshold for VEGF activation. This leads to phase 2 ROP. This process is demonstrated in Fig 2.
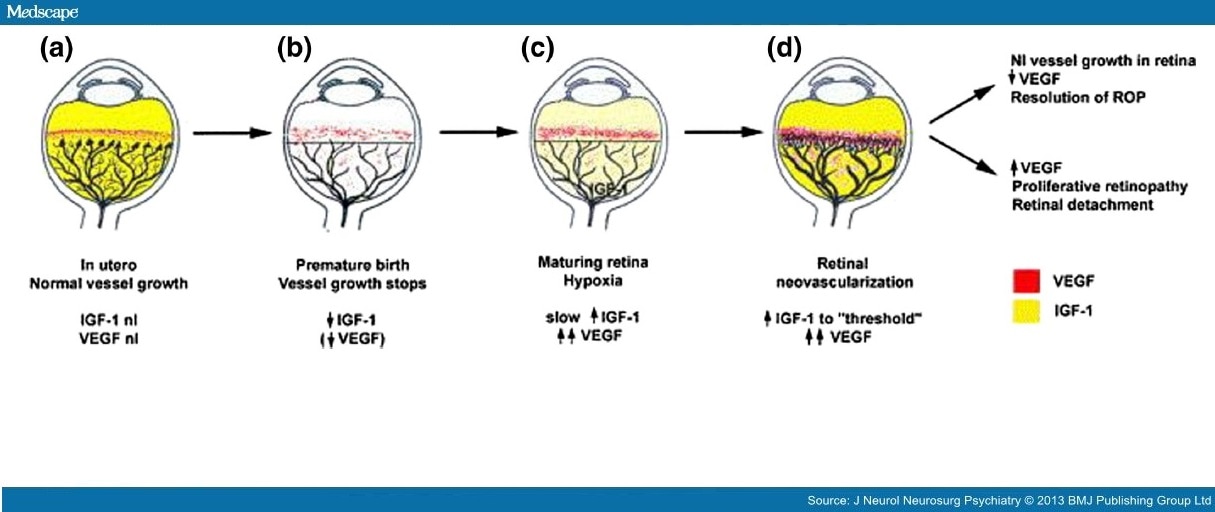
Figure 2.
Mechanism for retinopathy of prematurity (ROP) (Reprinted, with permission from Smith, L. (2003).9
Oxidative stress has long been implicated as a cause of ROP. Oxidative stress can be a consequence of inflammation as well as hypoxia/ischemia, hyperoxia, and reperfusion.[56] Preterm infants have higher levels of oxidative stress compared to term infants which is further complicated by an immature antioxidant system.[57]
Hypoxia alone can stimulate the production of tumor necrosis factor-alpha (TNF-α), a proinflammatory cytokine, which result in the breakdown of the retinal–blood barrier. Increased levels of TNF-α have been found in the retina of rats for up to 3 days after hypoxic exposure, inducing retinal ganglion cell death.[58]
Infection and ROP
All neonates are susceptible to infection because of immature immune systems, particularly the premature neonate, due to a delay or decrease in immune response to foreign antigens.[59] There is evidence that the exposure of the preterm neonate to infection and inflammatory mediators is associated with an increased risk for ROP.[11,60] Candida sepsis has been independently associated with an increase in the severity of ROP as well as the need for surgical intervention. A meta-analysis of eight studies found that systemic fungal infection in very low birth weight infants was significantly associated with ROP and severe ROP.[61]
Systemic Inflammation
Studies looking at maternal chorioamnionitis as an independent risk factor for ROP have not found a clear association.[54] Infants born to mothers with clinical chorioamnionitis with signs of systemic inflammation have been reported to have an increased risk for ROP.[62] Maternal systemic inflammation has been shown to decrease levels of IGF-1[62] which inhibits vascular growth by suppressing VEGF.
Oxidative stress has long been implicated as a cause of ROP. Oxidative stress can be a consequence of inflammation as well as hypoxia/ischemia, hyperoxia, and reperfusion.[56] Preterm infants have higher levels of oxidative stress compared to term infants which is further complicated by an immature antioxidant system.[57]
Hypoxia alone can stimulate the production of tumor necrosis factor-alpha (TNF-α), a proinflammatory cytokine, which result in the breakdown of the retinal–blood barrier. Increased levels of TNF-α have been found in the retina of rats for up to 3 days after hypoxic exposure, inducing retinal ganglion cell death.[58]
Lee and Dammann[54] reported that their series of epidemiologic studies support the hypothesis that prenatal, perinatal and postnatal systemic inflammation is an additional risk factor for ROP beyond immaturity and/or hyperoxemia. They found that prenatal combined exposure to systemic inflammation (SIRS) and chorioamnionitis (CAM) added to the risk of severe ROP[63] and that neonatal sepsis, oxygen exposure, and low gestational age were not only independent risk factors for ROP but also interact beyond additive and even multiplicative patterns.[11] They propose a possible pre-phase in the pathogenesis of ROP beginning prior to birth due to fetal inflammation as well as possible influences of neonatal inflammation due to early and late onset sepsis during phase I and II.
Nursing Implications
Nurses play a key role in the monitoring and management of the premature infant. Nurses must be educated in the need to maintain infant's oxygen saturations in an optimal range. It can be very difficult to maintain premature infants prone to periodic breathing and apnea of prematurity in a narrow oxygen saturation range. The nurse plays a vital role in infant positioning, activity, and oxygen titration to help maintain the infant in the defined range.
The bedside nurse is responsible for the prevention and detection of infection in the neonate. Infection prevention begins with appropriate hand hygiene. Hand washing has been identified as the most important action to avoid the spread of germs. Central line-associated blood stream infection (CLABSI) precautions are also important in the prevention of infection.[64] The nurse is responsible for the monitoring and detection of early sign of sepsis with prompt notification so the appropriate identification and treatment can be given.
The best prevention for the development of ROP would be to avoid premature birth. Because premature infants continue to be born, we must develop strategies for the provision of intensive medical care to improve outcomes for this population. Nursing actions that monitor oxygen saturations and oxygen delivery, as well as prevent and detect infection can aid in the prevention of ROP.
In summary, ROP is a vision-threatening disease that occurs only in premature infants. The process has been best described as occurring in phases with a suppression of vascular growth followed by a rapid proliferation. Although likely multifactorial, low birth weight, prematurity and oxygen use are strongly associated with an increased risk of the disease. There is increasing evidence that inflammatory processes related to perinatal infection and inflammation as well as postnatal sepsis also play a role in the pathogenesis of the disease that warrants further investigation.